KINESITHERAPY FOR RESPIRATORY DISEASES
The respiratory system consists of tissues and organs, providing pulmonary ventilation and pulmonary respiration. Respiration - a single process, which consists of three inseparable parts: external respiration, ie, gas exchange between the external environment, and pulmonary capillary blood, which occurs in the lungs, transport of gases by the system of blood circulation and blood of the internal (tissue) respiration, ie, gas exchange between blood and the cell, during which the cells consume oxygen and emit carbon dioxide. Basis of tissue respiration are complicated redox reactions, accompanied by the release of energy that is necessary for vital activity.
Human efficiency is determined mainly by the quantity of assimilated oxygen from the air passed into the pulmonary capillary blood and delivered to tissues and cells, which have three above-mentioned system. All of them are closely interconnected and have reciprocal compensation. Thus, when heart failure occurs shortness of breath, with a lack of oxygen in atmospheric air (eg, Medium) increases the number of red blood cells - oxygen carrier, for diseases of the lungs occurs tachycardia.
Respiratory system consists of the upper respiratory tract, bronchi, lungs, chest and breathing (intercostal, diaphragm, etc.), muscles (Fig. 77).
The level of lung function is determined by tissue oxygen need at the moment. In healthy people, from every liter vented air is absorbed about 40 ml of oxygen (so-called coefficient of oxygen utilization). In the atmospheric air contains 20.93% oxygen, 0,02-0,03% carbon dioxide.
In diseases of the lungs is disturbed respiratory function:
frustrated mechanics of breathing, which is associated with loss of elasticity of lung tissue, changes the rhythm of the phases of respiration, decreases mobility of the chest;
reduced ability to diffuse light, which leads to disruption of normal gas exchange between blood and alveolar air;
difficult bronchial patency by bronchospasm, bronchial wall thickening, increased secretion and mechanical bronchial obstruction with a large number of sputum.
It is known that a breach of respiratory function in diseases of the respiratory system is most often associated with changes in the mechanism of the respiratory act (violation of the right combination of inhalation and exhalation phases, the appearance of the surface and rapid breathing, discoordination respiratory movements). These changes often lead to a breach of pulmonary ventilation - a process that allows gas exchange between the outer and the alveolar air and supports the latest definition of partial pressure of O 2 and CO 2. Permanent and definite partial pressure of O 2 and CO 2 in alveolar air is necessary for the diffusion of oxygen from alveolar air into the blood of pulmonary capillaries. These processes perform the main task of the external respiration - the maintenance of normal oxygen tension and carbon dioxide in arterial blood. In pathology in the lung is one of the links that provide respiratory function begins to operate outside the norm, with resultant respiratory failure.
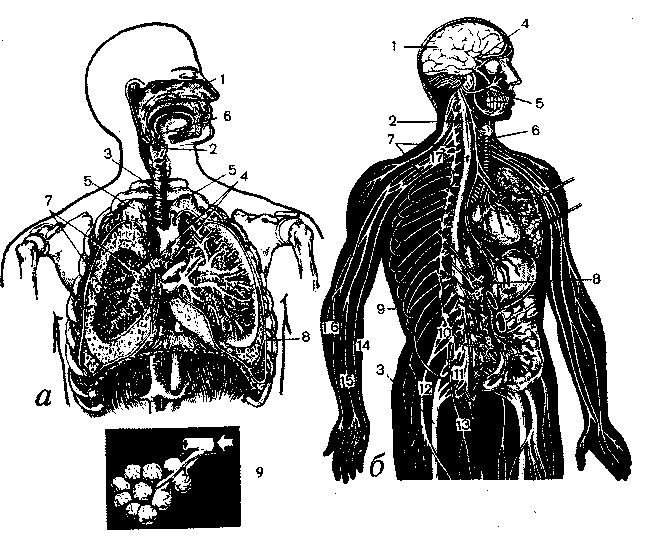
Fig. 77. And - the bodies of the thoracic cavity: 1 - nasal cavity, 2 - larynx 3
— Trachea 4 - bronchi, 5 - upper lung; 6 - oral cavity pharynx, and 7 - the branches of a lower-lobe bronchus, 8 - Diaphragm 9 - alveoli, b - peripheral and central nervous system: 1 - brain; 2 - dorsal brain: 3 - sciatic nerve; 4 - optic nerve, 5 - facial nerve; 6 - vagus nerve; 7 - hosts the sympathetic trunk, 8 - solar plexus, 9 - intercostal nerves, 10 - lumbar plexus; 11 - sacral plexus; 12 - femoral nerve, 13 - obturator nerve; 14 - ulnar nerve, 15 - the median nerve, 16 - radial nerve; 17 - brachial plexus
Violation of gas exchange in lung disease may result from reduction of their respiratory surface due to compression of the lung pleural exudate due to inflammation, the presence of infiltration, impaired bronchial patency, stagnation in the pulmonary circulation. Of pulmonary ventilation also contribute to poor expectoration of sputum, reducing trips diaphragm and chest, decrease contractility of respiratory muscles, the overall low physical activity the patient (physical inactivity) and other factors.
In applying the exercise of some compensation of respiratory failure can be achieved by improving the local ventilation (functioning pulmonary capillaries), so conditions are created to enhance gas exchange.
At rest, the man uses only 20-25% of the respiratory surface of lungs, the remaining 75-80% are included only in the case of intense exercise.
Functional unity of all parts of the respiratory system, ensuring the delivery of the tissues of oxygen, achieved by a thin neurohumoral and reflex regulation.
The role of respiratory muscles in the revitalization of breath during physical work.
The main objective of exercise therapy (or exercise) and pulmonary pathology is the restoration of impaired lung function.
It is known that the frequency and type of respiration vary depending on the position of the patient. So, in a horizontal position (lying on your back) the amount of chest corresponds to the phase of inspiration, the diaphragm is raised, the function of abdominal muscles is limited, exhaling difficult. In the prone position dominates the movement of edges of the lower half of the chest (more than the rear). In the initial position lying on their sides blocking the movement of the chest on the support side, the opposite side moves freely. Vertical position (standing up) - the best position to perform breathing exercises as well as chest and spine can move freely in all directions. In the sitting position prevails and inferolateral nizhnezadnee breathing, abdominal breathing is difficult, sitting with his back arched - verhnegrudnoe and abdominal breathing somewhat easier.
Pulmonary disease (pneumonia, bronchitis, pleurisy, etc.) worsens blood flow to the lungs and bronchi, the small tour (mobility) of the chest, shallow breathing, decreased respiratory muscle strength promote venous and lymphatic stasis and violates the expectoration of sputum. In addition, stagnation leads to the emergence of hypostatic pneumonia.
The use of exercise in pulmonary pathology is aimed at normalizing the blood and lymph circulation and thereby to eliminate stagnation in the lungs.
Systematic and early use of therapeutic exercises (MH) promotes the normalization of the frequency and depth of breathing, improve sputum, drainage function, the elimination of stagnation, etc. Massage neck area, chest, activation of respiration contribute to sputum discharge.
Efficacy of MH in patients with pulmonary pathology depends on the intensity (dosage) of the exercises, the ratio of respiratory and General developing exercises, starting position the patient, as well as age, gender, disease course and the functional state of the patient.
Pulmonary pathology inappropriate or hyperventilation (increase in pulmonary ventilation) or hypoventilation (a decrease of pulmonary ventilation, breath holding).
When performing MH depth of breathing should be adequate health patient's disease course, age and functional status of the organism.
Activation of respiration to the change of the original provision improves the drainage function of bronchi and increased depth of respiration. Exercise therapy helps to restore mobility edges (with operations in the lungs and heart), improving ventilation by increasing the microcirculation in the pulmonary capillaries, facilitates the work of the heart, strengthens the respiratory muscles, etc.